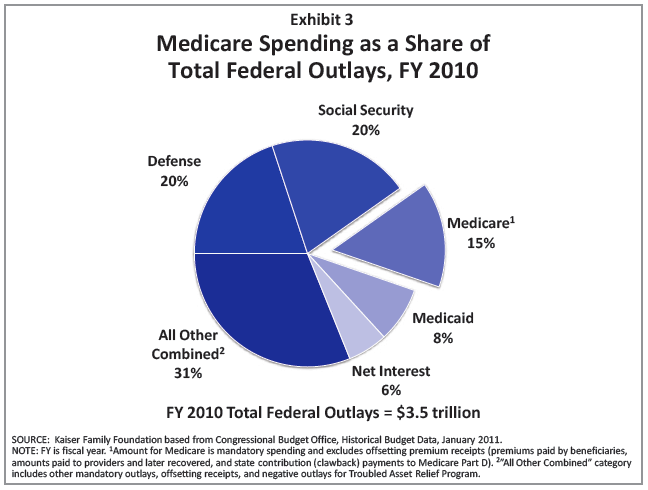
Reducing Medicare spending has been one of the focal points in the debt ceiling negotiations, and it was reported that the President is considering throwing the idea of raising the eligibility age for Medicare into the pot as part of a stone soup recipe that might get enough Congressional Ds and Rs to swallow the end product.
Increasing Medicare’s Eligibility Age is Bad Policy and Worse Politics
While increasing Medicare’s eligibility age to reduce spending makes simple arithmetic sense using the formula Spending = Number of People x Spending per Person, like almost everything in healthcare, what is simple is often 30 degrees wrong.…

{kind=link}