The debate about health reform has mostly focused on expanding insurance coverage and controlling costs. However, successfully improving the US healthcare system will require some long-term quality improving investments.
The stimulus bill (ARRA) included two such investments. The $1.1 Billion for Comparative Effectiveness Research has been widely discussed because it is important, and a very large percentage increase in the Federal Government’s spending in this area. But the ARRA bill also included $10 Billion to increase NIH’s funding.
The significance of the increased NIH funding is twofold: First, it will provide expansion of biomedical research related jobs. And second, it will help the NIH increase the work it does in translational research, which should help biomedical research build a better bridge over what the Parkinson’s Action Network and others have labelled the “Valley of Death.”
Valley of Death
The Valley of Death, as described by PAN at a briefing last week hosted by FasterCures, is the work required to turn basic lab research discoveries into treatments that help people. Some people call this “translational research,” and the NIH has been moving in this direction by funding institutional centers with Clinical and Translational Science Awards (CTSAs). The two major activities that occur (or don’t occur readily enough), in the Valley of Death are prototype discovery and design, and preclinical development. (See PAN’s graphic below.)
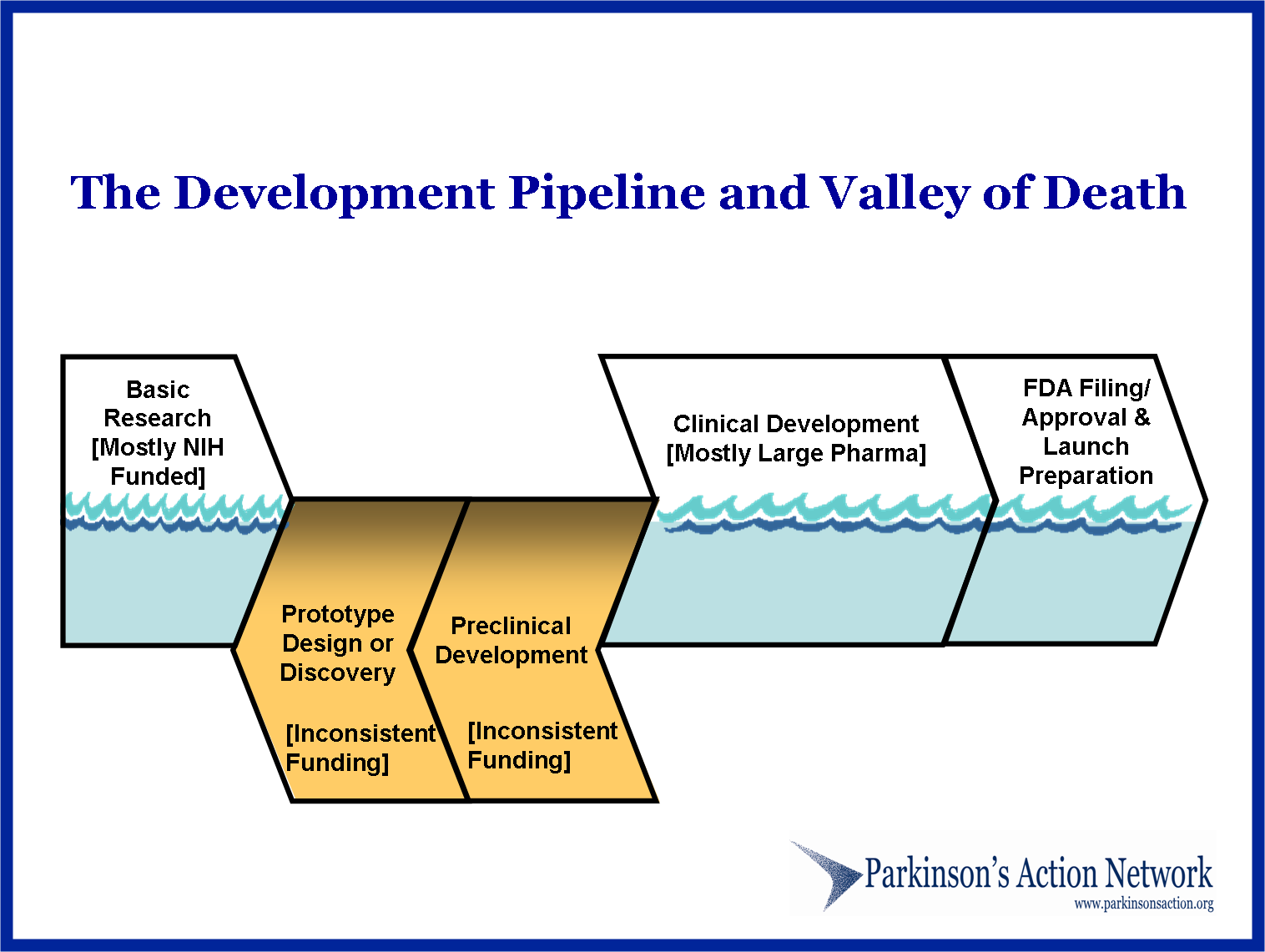
The Valley of Death is a real challenge because while these activities are vitally important for improving the quality of healthcare over the long run, the incentives for doing this work are smaller than for basic or fully applied research: In the private sector, there may be small incentives for translational work, but in academia the incentives may actually be negative because successes in this area garner little or no professional prestige or recognition, and more importantly, generally doesn’t attract research grants, i.e. money to support the researcher’s lab and the university.
A Bridge to Better Care
Filling in – or bridging – the Valley of Death, (feel free to pick your metaphor), is important for improving healthcare because there are so many serious conditions where current treatments are very inadequate. For example, Parkinson’s is one of many neurodegenerative diseases where existing treatments address some of the symptoms – and often only partially or temporarily – without effecting the course of the illness. Similarly, while significant advances have been made in treating cancer, those successes have been in select types of cancer, (with leukemia being one good example), or have made the treatments much easier for the patient. Both of these are valuable, but it is also worth noting the recent article discussing how survival rates for cancer haven’t really increased over the last several decades.
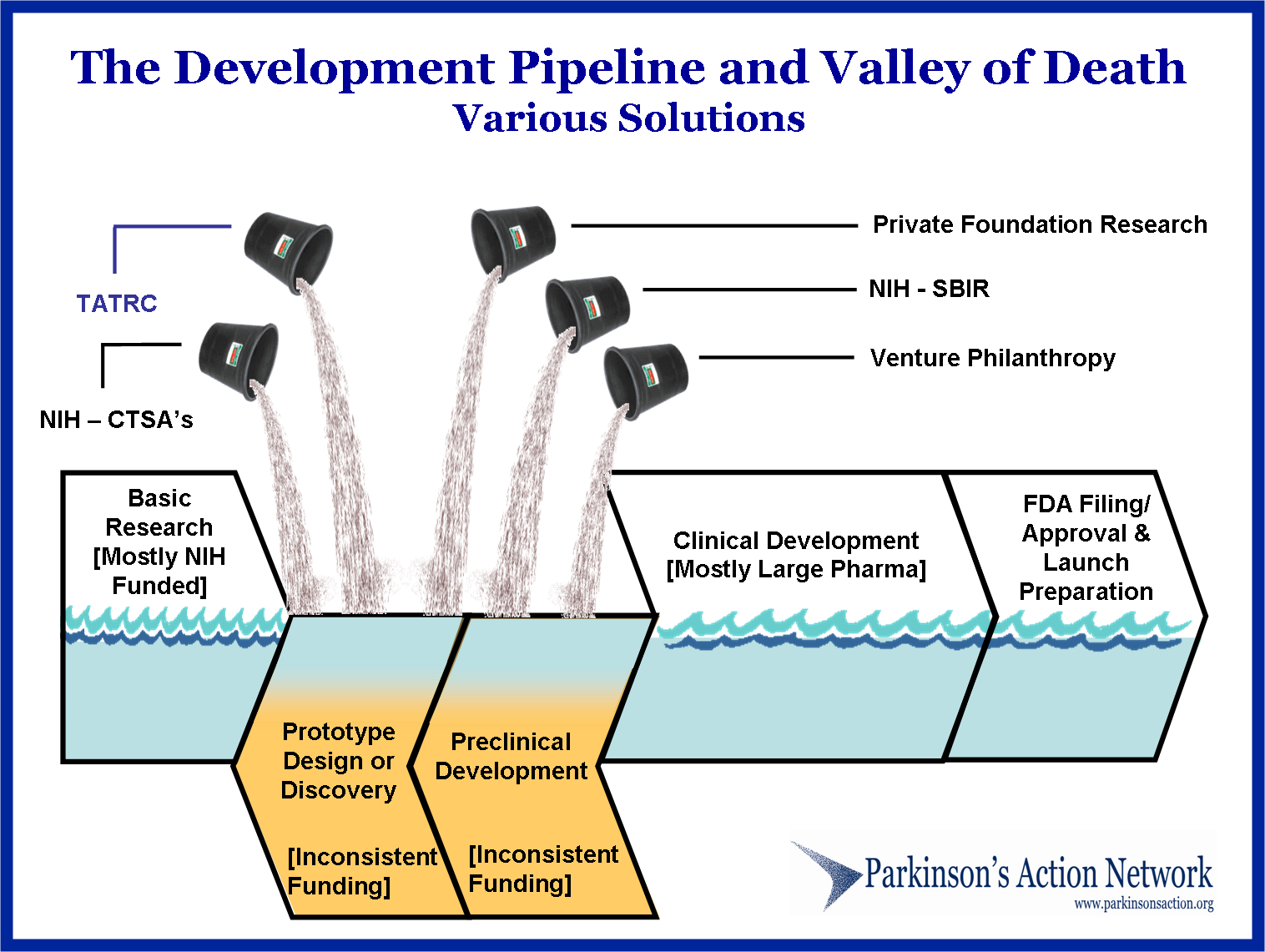
The cure for this problem is clearly more (and better) research and development…. and the translational work that bridges the two. (Perhaps we should talk more about increasing R&T&D, rather than just R&D?) PAN’s description of how to do this is sophisticated and multifaceted. As their illustration below shows, not only are the NIH’s CTSAs and SBIR programs important for helping institutions and individual researchers push forward with more translational work, but other parts of the solution include DoD’s Telemedicine & Advanced Technology Research Center, and private foundations and venture philanthropy.
Increasing funding for translational work through all these sources may help build a bridge, (of fill in the Valley), but translational work will also benefit by greater coordination of efforts. At the institutional level that is part of the role of the CTSA’s, but there could also be more coordination and emphasis of translational work at the NIH itself – which is why PAN is recommending the NIH conduct an analysis and present their own recommendations for improving the translational activities of NIH funded research programs.
Institutional researchers could also benefit by having more resources about the nuts and bolts of translational work – like how to structure research and information so that it will be readily usable for filing an IND with the FDA. Universities already have Technology Transfer/Licensing offices that serve the dual function of licensing university generated research to private companies for commercialization and ensuring that the university receives fair compensation for the company’s use of these discoveries – which is required by the Federal Bayh-Dole Act. Perhaps universities should also have offices that work to educate their researchers about translational activities to help them plan their research so that the information they generate will be more readily usable by those farther down the development pipeline?
This is clearly not an easy nor readily obvious task. At the FasterCures/PAN briefing last week, someone told a story about an academic researcher who experienced a 2 year delay in moving their discovery along the development pathway because they didn’t understand the information that would be needed.
Rather than make specific recommendations about how to improve the situation for basic researchers, I’ll just note that the Bayh-Dole Act managed to get every institution receiving Federal grants to create a Technology Transfer/Licensing office. It seems that every institution could also have a Office of Translational Research Assistance too. How to structure the funding or financial incentives for this could be complicated, but certainly not impossible. And given that we are spending tens of Billions of tax dollars on biomedical research, we should also be doing everything we can to make sure that the discoveries coming out of that research gets translated into better treatments for patients ASAP. Delays because academic researchers don’t want to pitch their careers into the Valley of Death, shouldn’t be a tolerated part of the structure of our biomedical research system – which, as I’ve previously discussed, is one of the four spheres comprising our entire healthcare system.

The government should not compel doctors and hospitals to participate in a public plan just because they participate in Medicare.
This chess match will continue for a while, but keep in mind the Democrats are in the position to end the game their way this fall through the budget resolution passed last week allowing them to consider healthcare reform legislation without the threat of a filibuster.
[…] A couple of weeks ago I wrote about translational research barriers – also known as the “valley of death” – and some larger, national public and private programmatic solutions. This week’s Mass High Tech newspaper has a cover story about how Children’s Hospital in Boston created a $1 Million fund to help their researchers bridge that gap to take their discoveries into the development process that can actually lead to better patient care. […]