The Medicare Payment Advisory Commission released its annual report to Congress on Friday. In chapter 2 of its report, MedPAC makes two significant proposals for improving the financial incentives for primary care providers.
Great Incentives for Primary Care Practitioners Not Just Primary Care Services
First, it recommends changing Medicare’s reimbursement system for “evaluation and management” (E&M) services. While last year Medicare increased payments for E&M services, they couldn’t differentiate between types of physicians providing these E&M services, i.e. the Medicare system doesn’t distinguish between a family physician and a cardiologist if they are providing the same type and level of intensity of service.
Therefore, MedPAC recommends that a subset of primary care related E&M services, (e.g. office visits, home visits, long-term care patient visits), provided by clinicians who meet a minimum percentage threshold of a clinician’s total Medicare billing, (and thus would be identified as being “primary-care-focused practitioners”), should receive higher Medicare payments. (MedPAC choose to identify primary care clinicians based upon a percentage of primary care services – rather than specialty designation – because it would be administratively simpler and ensure that the incentives would be directed towards clinicians actually providing primary care services.)
The specific recommendation from the MedPAC report is:
The Congress should establish a budget-neutral payment adjustment for primary care services billed under the physician fee schedule and furnished by primary-care-focused practitioners. Primary-care-focused practitioners are those whose specialty designation is defined as primary care and/or those whose pattern of claims meets a minimum threshold of furnishing primary care services. The Secretary would use rulemaking to establish criteria for determining a primary-care-focused practitioner.
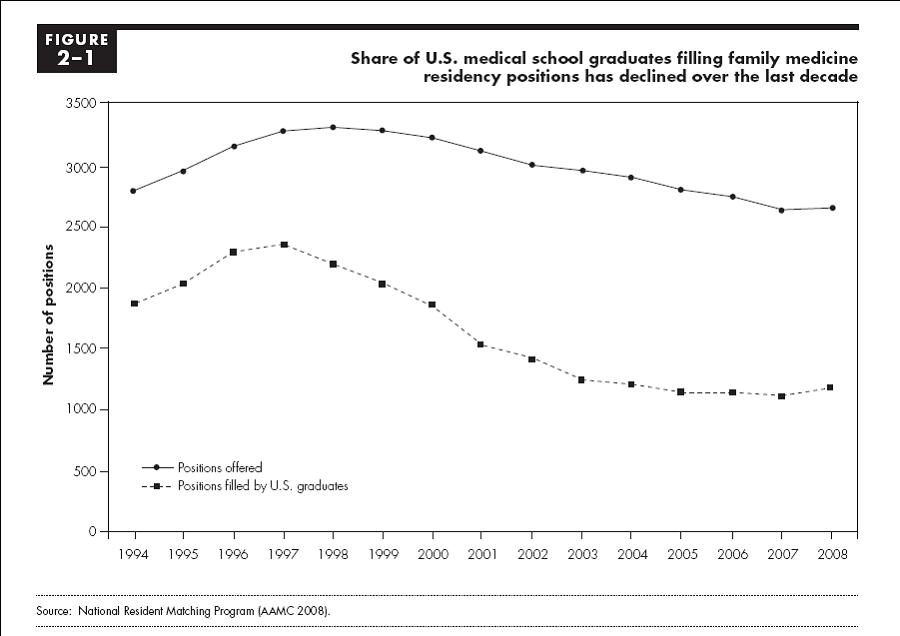
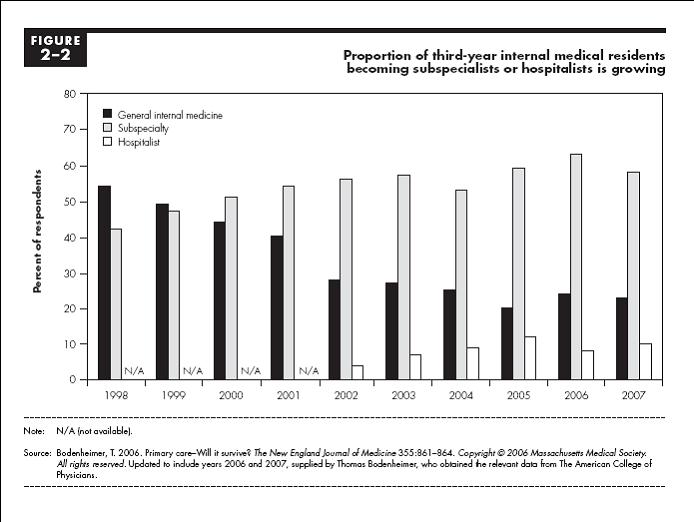
This is a sea-changing proposal in that it seeks to differentiate how Medicare Part B reimburses primary care providers versus subspecialists – and thus makes Medicare Part B payments more granular than was done when the RBRVS system was first installed in the early 1990s. (Back then, the fight was between so-called cognitive and procedural services.) This refinement will enable Medicare in the future to use its payment system as a more managerial tool for shaping the healthcare delivery system to increase the supply and access of primary care practitioners. The need for such changes is evident by the shrinking number of medical school graduates going into primary care:
However, because the proposal is intended to be budget-neutral it explicitly pits the financial interests of primary care practitioners against subspecialists, which means that the subspecialists will not eagerly welcome these changes to Medicare since they would be getting a smaller piece of a same-sized pie. (Note – MedPAC’s analysis shows that using the a cut-off of 65% of primary care services for clinicians to receive a 10% increase in payments for these services, would increase reimbursements for these services by a total of 6.2%, and would require a reduction for all other services of 0.9% to achieve budget neutrality.)
Build a Medical Home
MedPAC’s second proposal to promote more primary care is to increase the number of Medicare beneficiaries with medical homes.
Medical homes are the latest name for initiatives to give patients a single clinical practice or practitioner to ensure that their care is coordinated with the goal of improving the quality of care, and controlling costs by avoiding unnecessary complications and unnecessary testing. Medical homes are particularly important for people with chronic conditions for ensuring appropriate compliance with recommended treatments, disease monitoring and preventive testing. As the MedPAC report states, “Unlike the current fee-for-service (FFS) payment system, which emphasizes treatment for acute conditions and face-to-face care, medical home programs encourage practitioners to coordinate their patients’ care between visits and among providers. In improving care continuity and coordination, medical homes can enhance the role of primary care practice … [and] … increase our health system’s quality and efficiency.”
Medical homes are not new concept, as care coordination has been discussed since the original concept for HMOs several decades ago. Recently they have been promoted by primary care associations, and Medicare will start a medical home demonstration project in January 2009. MedPAC’s proposal builds off of the planned pilot, and would provide additional monthly payments to medical home practices providing the care coordination services. (Signing up with a medical home would be voluntary for Medicare beneficiaries and they would not have to pay any additional co-payments or premiums.)
MedPAC’s specific medical home proposal, which goes beyond the planned pilot project, is:
The Congress should initiate a medical home pilot project in Medicare. Eligible medical homes must meet stringent criteria, including at least the following capabilities:
- furnish primary care (including coordinating appropriate preventive, maintenance, and acute health services) [and medication management]
- conduct care management
- use health information technology for active clinical decision support
- have a formal quality improvement program
- maintain 24-hour patient communication and rapid access
- keep up-to-date records of beneficiaries’ advance directives, and
- ‘maintain a written understanding with each beneficiary designating the provider as a medical home.
Medicare should provide medical homes with timely data on patient utilization. The pilot should require a physician pay-for-performance program. The pilot must have clear and explicit thresholds for determining whether it can be expanded into the full Medicare program or should be discontinued.
MedPAC recommends an enhanced pilot project – rather than a national initiative -because there are administrative and technical factors that still need to be worked out, including, how to structure monthly payments to medical homes, and how to provide medical homes information about services provided to their patients by other providers so they can do care coordinating. The good news proposals for specialist physicians in MedPAC’s is that the pilot is not being proposed as budget neutral, but would cost between $250-750 million over 5 years.
Conclusions
Most experts think these proposals will be effective in improving the healthcare delivery system in the US, and I agree – provided that they are structured and implemented so they actually change the actions of physicians and patients. To be successful they need to change physicians’ practice patterns to focus more on primary care and care coordination, and to change patients’ behaviors so they use their primary care clinicians for more of this care management. In addition, as is reflected in the charts above, these proposals face the logistical challenge of finding enough primary care clinicians to provide these services. These changes will take time – it takes years to alter patient-physician relationships, shift how physicians practice or increase the supply of primary care clinicians – but this is not a reason for further procrastination.
p.s. I’m writing this from the road, so my editing and grammar may be somewhat deficient – my apologies.

[…] the general consensus being that we have a shortage of primary care clinicians, cutting Medicare payments to physicians in underserved areas seems truly unwise. And doing it at […]