Discussion of health reform this year often touches upon how the process and substance are so different than what occurred in 1993-4, even though many of the people engaged in the current effort were also involved then too.
Historical events are clearly important for setting the political and policy environment for any legislation, and in healthcare there are very clear examples of stagger-stepping to success:
At the Federal level, health insurance/coverage laws and proposals date back to the 1930s:
- National health insurance for the elderly was supposed to be the second part of a new social safety net – after the creation of Social Security
- Medicare and Medicaid were created in 1965.
- In the 1980s and 1990s, Medicaid was repeatedly expanded in small increments, and in 1997 the State Children’s Health Insurance Program was built on top of Medicaid.
- Massachusetts’ coverage expansion laws:
- Universal Coverage Law in 1988 (delayed and repealed in 1996)
- Major Medicaid Waiver in 1996
- Revised Medicaid Waiver and State Law for Insurance Coverage Expansion in 2006
Medicare expanded outpatient prescription drug coverage:
- Medicare Catastrophic Coverage Act in 1988 (repealed in 1989 before implementation)
- Medicare Cancer Coverage Improvement Act added very limited coverage for outpatient prescription drugs to treat cancer in 1993
- Medicare Prescription Drug Improvement and Modernization Act in 2003 added the new Part D outpatient prescription drug benefit and a temporary prescription drug discount card program. (The discount card program was in effect from June 2004 through 2005, and the Part D benefit started in 2006.)
Learning from the Crazy Quilt
All these laws have created a crazy quilt structure, but this history also has lessons for the current Federal health reform efforts: First, repeated attempts at taking on an issue can lead to success. Second, incremental success, (or success in incremental steps), may be achievable when larger changes are not. And third, compromise and inclusion of various approaches and provisions in a final product can mean the difference between stalemate and success.
This last point is why I think that the Medicare Modernization Act and Massachusetts’ 2006 experience are very important for the current debate. In both cases, various compromises were made – on both policy and politically related aspects of the legislation. In Massachusetts, the biggest compromises involved the inclusion of both individual and employer mandates, as well as primarily using private insurance for expanding insurance coverage. Similarly, in the MMA’s Part D program, the estimated costs was capped at $400 billion over 10 years, private insurance was used as the vehicle for providing the new drug benefit, and the standard benefit was biphasic to limit government costs while providing a significant benefit to the few individuals with very high drug costs, and a limited benefit to many more people. (See graphic of the 2009 standard benefit below.)
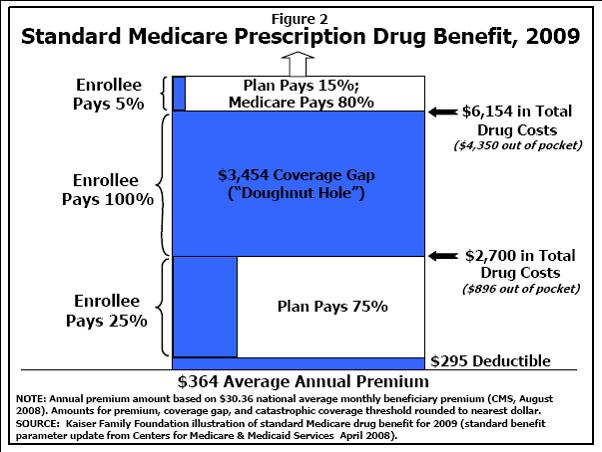 Source: Kaiser Family Foundation Fact Sheet “Medicare Prescription Drug Benefit,” March 2009
Source: Kaiser Family Foundation Fact Sheet “Medicare Prescription Drug Benefit,” March 2009
Current Efforts Have Learned from History?
The Obama administration’s position and actions have been consistent with these lessons, and it is seen in their willingness to discuss all possible options for moving towards universal coverage, containing costs and improving quality. However, they are also clearly constrained by exploding budgetary pressures – particularly in the near term. While it is possible that the bailout funds, (and government purchase of “toxic assets”), will eventually create positive returns, that will certainly take several/many years, and the need for health reform can’t wait that long.
Therefore, the successful efforts in Massachusetts and with the Medicare Prescription Drug Benefit demonstrate the importance of compromise and cobbling together positions supported by various factions within a single law so that it will have broad support – which facilitates both passage and implementation. After all, a baseball player improves his batting average by learning how to hit and by studying great hitters like Ted Williams, rather than by learning how to strike out, or by studying Mario Mendoza’s swing.