A recent Boston Globe article about a possible legal challenge to Masschusetts’ health reform initiative indirectly raised one of the most stubborn challenges in health reform: The Federal ERISA law. (See below for more about ERISA.)
The contentious issue in Massachusetts is a proposal to require employers to both pay at least 33% of full time employees’ health insurance premiums and ensure that at least 25% of their employees are covered by their health plan. (The current requirement is that they do one or the other.) So why should this difference be the basis for a law suit? Actually, there isn’t really any legal difference. In either case, an employer that provides health benefits to their employees by self-insuring, (rather than directly buying coverage from a health insurance company), could sue based upon the Federal ERISA law that regulates employee benefits.
The real difference between the proposal and the current law is political and philosophical rather than legal – employers are willing to live with the current either/or requirement, but don’t want to be pushed down a slippery slope where the coverage requirements and/or the small penalty of $295/employee for failing to meet the requirements are increased. And their legal backup is ERISA.
So What is ERISA? (Without going into too much detail.)
ERISA stands for the Employment Retirement Income Security Act of 1974, and it is a Federal law that governs how companies provide benefits to their employees. The law is overseen by the Department of Labor, and was originally designed to ensure that pension benefits were properly managed and funded. However, it also encompasses health benefits – but only for companies that provide the benefits themselves by self-insuring rather than purchasing health insurance for their employees from insurance companies. The result is that ERISA mostly applies to larger companies which typically self-insure for several reasons:
- They don’t have to comply with state health insurance mandates – which is one reason why large companies can reduce their health benefit costs by self-insuring
- Since many large companies have employees in more than one state, by self-insuring, they can operate a single health benefits plan – under what is called an ERISA exemption – rather offer different health insurance options in each state based upon the states’ insurance laws
- By accepting the financial risk of self-insuring, they can also receive any financial rewards from controlling health care spending. This also gives them incentives to keep their employees healthy as well as productive
ERISA is a Linchpin for Federal or State Health Reform
ERISA is a crucial part of health reform that is not very well appreciated and generally not discussed outside of very wonkish circles – which is probably why the Boston Globe article doesn’t even mention it.
At the State level – as in Massachusetts – ERISA theoretically precludes state governments from placing requirements on self-insured company’s health benefits programs. However, ERISA does regulate how the benefits are provided, has requirements about providing information to employees about their benefits – aspects that are consistent with the law’s original focus on pension benefits – and has four coverage mandates:
- Non-discrimination against pregnancy as a medical condition
- Hospital length of stays for women following delivery: 48-hours or 96-hours following a Cesarean
- Parity between mental health and other benefits
- Reconstruction following mastectomy
ERISA has also been changed to require that companies continue to offer health coverage for a limited amount of time to employees after they leave the company (COBRA in 1986), and to limit or ban the exclusion of pre-existing conditions or other factors that might predict their need for future health care needs (HIPAA in 1997).
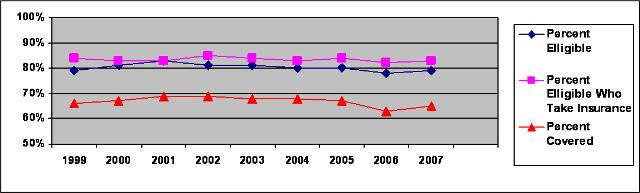
ERISA coverage requirements has rarely been modified because of the lack of any clear consensus for what changes should be made, and the concern that adding coverage mandates to ERISA would increase costs without expanding the number of people with insurance or improving quality. In essence ERISA is a major obstacle for health reform because it regulates one of the largest and most stable parts of the employer-based health insurance system. For example, the Kaiser Family Foundation’s annual survey of employers has shown that 98-99% of companies with more than 200 employees have offered health insurance to their employees every year since 1999. Similarly, the percentages of employees who are eligible and who chose insurance coverage have remained relatively stable from 1999-2007:
Large Companies (>199 employees) Offering Health Benefits:
Eligibility, Take-Up and Coverage Rates
[It should also be recognized that health insurance costs are a significant factor for large companies to outsource jobs to small companies or independent contractors here in the US, or to send those jobs overseas to companies that have cheaper labor costs.]
The ERISA Chasm
ERISA is a huge uncrossed chasm for health reform because virtually any state law that places requirements on the health benefits provided by self-insured companies could be subject to a Federal lawsuit. And at the Federal level – as noted above – nobody has come to a consensus as to what should be done, except for some chipping at the edges with worthwhile requirements. In addition, the Committees with jurisdiction for ERISA generally have not made ERISA health benefit issues a high priority: In the Senate, jurisdiction for ERISA is shared between the Finance and the Health, Education, Labor and Pension Committees. Each of these committees has significant other responsibilities, including Medicare, Medicaid, biomedical research and the FDA. And in the House of Representatives, the Education and Labor in the House of Representatives has jurisdiction for ERISA, which is really their only health related area of authority.
ERISA’s Implications for Obama and McCain Health Reform Proposals
The importance of ERISA and its Federal oversight over all self-insured employer provided health benefits raises the question of how the plans of Senators Obama and McCain would be effected by ERISA?
Senator Obama’s plans clearly call for more Federal regulation of health insurance which could significantly change how health benefits are provided to employers. This avenue for creating a more stable system for health insurance/benefits changes would have to involve ERISA. However, his proposals explicitly state that individuals could keep the coverage they now have – which would likely mean limited changes to ERISA, and those changes might not raise too many objections from the large business community.
Senator McCain’s plans are based upon shifting the purchase of health benefits from the company to the employee by moving the tax deductibility from the company to the individual. (It appears that there would also be a dollar limit on this deduction, and in essence also shifting from the general current situation of health benefits being a “defined benefit” to being a “defined contribution” – something that happened with many pension plans in the last ten years as a means for companies to control or limit their future financial liabilities.) If a McCain plan required everyone buy their own insurance from insurance companies, then changes to ERISA wouldn’t be required, but it might lead to much more state legislative and regulatory action as millions more people become subject to state laws for both insurance company marketing and plan design. In addition, one selling point used for McCain’s campaign positions, is that it would enable employees to take their health insurance with them as they went from job to job. For that to be true across state lines, then tremendous changes to ERISA would be necessary – and probably much more than under the proposals that might come from an Obama Administration.
Conclusions
Sorry about the very long post, but as the title states, ERISA is truly an unbridged chasm. Many health reform proposals have raced up to its brink only to suddenly stop short at the edge of the ERISA cliff – sort of like the comedy Westerns of the 1950s where the rider gets pitched over the head of the horse into the canyon. In this analogy, perhaps the public and the politician are the horse, (I’ll let you decide which half is which), and the proposal is the rider – which gets lost in the depths of the canyon because the horse can’t find a way across.
For significant health reform to be achieved, all constituencies and stakeholder groups need to reach some consensus to build a bridge across the ERISA chasm. Otherwise, no action will likely continue to be everyone’s second and fall-back option.

ERISA and Self insured plans skirt MA State mandate CMR 37.08 which protect people from being overcharged for infertility. ERISA and self insured plans reimburse as little as $5000 lifetime max with a 50/50 cost split.
[…] PPS: Dr. Michael Miller has just posted a valuable essay on ERISA and national reform, here. […]